
Purpose
The purpose of this brief is to support pediatric and family medicine care teams in adopting measures to better support the needs of children ages 0-5 and their families. This topic brief defines behavioral-developmental health screening and response, outlines its benefits, and provides strategies for implementing it in pediatric and family medicine practices for children ages 0-5.
Definition
Behavioral-development health screening and response is an approach to pediatric primary care where care teams administer screenings to identify behavioral health symptomatology, developmental delays, adversity, and health-related social needs and then provide brief interventions and referrals, if needed. Behavioral-developmental health screening and response aims to provide families with young children the assistance and knowledge needed to promote foundational brain development during the first 5 years of life. This approach reflects the scientific understanding of how early childhood experiences, both positive and negative, can significantly impact a child's brain development and subsequent long-term health.
The formative years of childhood, particularly from birth to age five, play a vital role in shaping a child's cognitive, emotional, and social development. Ninety percent of brain development occurs during these years, and neuroplasticity—the brain's ability to form and reform neural pathways—is at its peak.1,2
A child's early experiences significantly influence the development of their brain and their outcomes in life.3 Adverse childhood experiences (ACEs), such as violence, neglect, and parental substance abuse, can cause toxic stress and disrupt a child's development of executive functioning, neuroplasticity, emotional regulation, and interpersonal skills.4 This disruption can potentially increase the risk of developmental delays, learning difficulties, mental health and substance use disorders, and other long-term health issues in adulthood.5,6,7,8,9,10
Compounding these disruptions are unmet health-related social needs (HRSN) (PDF – 248 KB), such as food, diaper, or transportation insecurity, which can further exacerbate stress on both children and parents. For example, optimal nutrition during the first 1,000 days of life is essential for brain development. Deficiencies in key nutrients, such as iron, zinc, and choline, can lead to lifelong cognitive impairments.11 Diaper insecurity is linked to increased risk of diaper rash, urinary tract infections, and stress for mothers and can hinder access to early intervention services, further impacting child development.12,13
Positive childhood experiences (PCEs) (PDF – 607 KB), such as having strong, supportive relationships, a sense of belonging, and having a sense of safety can mitigate the negative effects of ACEs and promote positive health outcomes for children throughout their lives.14,15,16,17 When children experience PCEs, they develop coping and problem-solving skills and build and nurture their ability to face, overcome, and be strengthened by adversity—also known as resilience.18,19 Much like a seesaw or balance scale, accumulating PCEs tilts the scale towards positive outcomes and helps to offset the negative outcomes caused by ACEs and other adversity. Meanwhile, resilience acts as a fulcrum, shifting the balance point of the scale in favor of positive outcomes.20
Behavioral health providers often describe the cumulative impact of a child's early experiences using the metaphor of an “invisible backpack.” In this metaphor, every child carries an invisible backpack that contains risk factors, such as ACEs and prolonged stress, and protective factors, such as safe environments and supportive relationships, that shape their current and future health and well-being.
Pediatric and family medicine care teams are uniquely positioned to identify and address the contents of this backpack, particularly for children ages 0-5. The continuity of the well child visit model provides care teams with the opportunity to conduct regular screening for ACEs and unmet HRSN such as food insecurity, diaper insecurity, transportation challenges, and barriers to accessing childcare and pre-school.
The American Academy of Pediatrics recommends that pediatric and family medicine practices use well child visits to screen for developmental delays, adversity, and HRSN, as well as give age-appropriate information and advice to parents or caregivers about the expected growth and development of their children—referred to as anticipatory guidance—and to partner with families to build resilience and promote safe, stable, and nurturing relationships.21,22 By providing these brief interventions, as well as referrals to behavioral health, early intervention, social services, and other community supports and assistance, care teams can promote optimal outcomes for children.23,24,25 However, approximately 32% of pediatricians do not usually ask or screen for ACEs.26
Traditional healthcare for infants and young children (ages 0-5) has primarily focused on physical health.27,28,29,30 Behavioral-developmental health screening and response includes components to address social, emotional, and behavioral factors like adverse childhood experiences (ACEs) and health-related social needs (HRSN) in children ages 0-5 in pediatric and family medicine.
While there is not yet an established and validated framework for behavioral-developmental health screening and response, several practices and health systems have implemented their own models.31,32,33,34 The Center for the Study of Social Policy has an extensive list of programs (PDF – 327 KB) implementing behavioral-developmental health screening and response models. Based on a review of these programs, Table 1 (below) summarizes and defines nine common components being implemented in these models.
Component | Description | |
|---|---|---|
1 | Trauma-informed approach |
|
2 | Two-generation approach |
|
3 | Provider/staff training |
|
4 | Anticipatory guidance |
|
5 | Parent/caregiver education |
|
6 | Team-based care |
|
7 | Standard workflows for screening and response |
|
8 | Connection to community resources |
|
9 | Data utilization |
|
How each practice or health system chooses to implement these components is flexible and customizable based on available resources, staff expertise, and specific organizational goals. To illustrate the different ways behavioral-developmental health screening and response can be implemented in different settings, a sample of those models is listed below.
- In the Developmental Understanding and Legal Collaboration for Everyone (DULCE) model, Family Specialists (community health workers trained in early child development, relational approaches to family-centered care, and concrete support problem solving) work with families of children ages 0 to 6 months in pediatric medical homes. Practice staff and Family Specialists collaborate to identify where in the workflow the Family Specialists will conduct screening and how to communicate the responses. The Family Specialists attend well-child visits and build trusting relationships with the families. During the visits, they provide anticipatory guidance and direct education and support. They also conduct screening for employment security, food security, intimate partner violence (IPV), financial supports, transportation, mental health/caregiver depression, housing stability, housing health and safety, and utilities. Each Family Specialist works with a DULCE Interdisciplinary Team comprised of a clinical administrator, a pediatric or family medicine provider, a legal partner, and representatives from the early childhood and mental health systems to review screening results and connect families to the services and resources they need.
- In the Family Connects Model, registered nurses conduct up to three home visits with families with newborns during the first three weeks after birth. During these visits, Family Connects nurses perform physical health assessments; conduct screenings for postpartum depression, substance use, and IPV; and offer anticipatory guidance and direct education and support. Family Connects maintains a customized, HIPAA-compliant database that serves as a comprehensive case record system. The nurses use this system during home visits to document clinical interviews and screening results, identify potential referrals, and ensure that referrals are utilized by families. After home visits, they provide reports to the families' pediatric primary care providers to create a bridge to ongoing care.
- In the HealthySteps model, HealthySteps Specialists (community health workers trained in child development and behavioral health promotion and prevention) join pediatric primary care practices. They collaborate with practice staff to develop workflows for conducting routine physical, cognitive, language, social-emotional, developmental, and behavioral screenings with families with children ages 0-3. HealthySteps Specialists also offer anticipatory guidance, health education, and parent coaching. When referrals are needed, they collaborate with community organization and local agencies to help families successfully access their resources and services. HealthySteps also offers a family support phone line that families can call with child development, parenting, and behavior-related inquiries.
- In the Parent-focused Redesign for Encounters, Newborns to Toddlers (PARENT) model, Parent Coaches (community health workers trained in comprehensive early childhood preventive care) join care teams in pediatric primary care practices. Families with children ages 0-3 complete a web-based questionnaire prior to attending their well child visits to indicate their priorities for the visit and identify any developmental or behavioral concerns or HRSN. Parent Coaches join the well child visits and provide anticipatory guidance, psychosocial assessment and referral, and developmental/behavioral surveillance, screening, and guidance. Parents also receive automated text messages that provide anticipatory guidance, health education, developmental tips, and reminders.
- In the Environment for Every Kid (SEEK) Model, pediatric and family medicine care team members complete online training on seven major behavioral health issues, as well as motivational interviewing, relationship building, and barriers to engagement. Prior to well-child visits, parents and caregivers with children ages 0-5 complete a brief questionnaire that screens for parental wellness, home safety, child behavior, food insecurity, and other HRSN. The questionnaire is usually completed on a clipboard in the exam room but can also be completed electronically and integrated into an electronic health record. During well child visits, care team members use motivational interviewing to partner with families, identify risk factors, and develop personalized plans. Families receive post-visit handouts that reinforce key topics discussed during their visits, as well as referrals to community resources and local agencies, if needed.
Current evidence indicates that behavioral-developmental health screening and/or response can improve screening rates, identification of adversity, referrals to services, and patient satisfaction.35,36 Multiple randomized control trials found that behavioral-developmental health screening and response models have resulted in:
- Reduced healthcare utilization, including fewer emergency department visits
- Better adherence to well-child schedules
- Decreased use of negative parenting strategies
- Improved developmental and behavioral healthcare
Research on the impact of behavioral-developmental health screening and response on child and family health outcomes is promising but remains limited.37 Table 2 (below) summarizes statistically significant outcomes data for children and families from randomized control trials conducted on the five behavioral-developmental health screening and response models described in the previous section.
Model | Study | Age Range | Practice Type | Outcomes Data for Children and Families |
|---|---|---|---|---|
Developmental Understanding and Legal Collaboration for Everyone (DULCE) | Sege et al. (2015)38 | 0-6 months | Safety-net hospital | Compared to the control group, intervention infants were:
|
Family Connects Model | Dodge et al. (2013)39 | 0-12 months | Community hospitals | Compared to the control group, intervention families had:
|
Goodman et al. (2019)40 | 0-24 months | Community hospitals | Compared to the control group, intervention families had:
| |
Dodge et al. (2019)41 | 0-24 months | A university hospital | Compared to the control group, intervention families:
Compared to the control group, intervention mothers had:
| |
HealthySteps | Minkovitz et al. (2001)42 | 0-3 years | Pediatric primary care clinics | When compared to the control group, intervention parents were:
At the 5.5-year follow-up, when compared to the control group, intervention families were:
|
Parent-focused Redesign for Encounters, Newborns to Toddlers (PARENT) | Coker et al. (2016)44 | 0-3 years | Pediatric primary care clinics | Compared with the control group, intervention parents were:
|
Coker et al. (2023)45 | Multisite federally qualified health centers | Compared with the control group, intervention parents were:
Compared with the control group, intervention children were:
| ||
Safe Environment for Every Kid (SEEK) Model | Dubowitz et al., (2009)46 | 0-5 years | University-based resident primary care clinic | Compared to the control group, intervention families:
|
Dubowitz et al. (2012)47 | Pediatric primary care clinics | Compared to the control group, intervention mothers reported:
|
Pick a start date and work backwards from there, building in time to garner buy-in and get your practice or system ready. Consider the following questions:
- Who will champion this effort? Determine a team leader who will facilitate and sustain this behavioral-developmental health screening and response effort.
- Whose buy-in do we need? Build support with leadership and clinical and administrative staff in each area of your practice or system. Start thinking about patient and family engagement.
- What can we reasonably achieve? You will not be able to address every need identified during screening, so what can you realistically do and achieve given your practice or system's resources and capacity?
TIP: Create initial aim statements.
Aim statements are written descriptions of the accomplishments you expect from your efforts. These statements can help you organize and articulate your goals. You can use this aim statement worksheet (PDF – 215 KB) or the formula and examples below to get started.
By [DEADLINE], we will [OUTCOME/ACTION] for [INTENDED POPULATION] by [GOAL] (as measured by [DATA SOURCE]).
Examples:
- From January 1st, 2025 to December 31st 2026, we will use the Safe Environment for Every Kid (SEEK) Model to conduct screening and response for adversity and positive child experiences in 75% of children ages 0-5 (as measured by SEEK Medical Record Review).
- By December 31st 2026, we will increase our yearly developmental screening rates using the Survey of Wellbeing of Young Childhood for children ages 0 to 5, from 0% to 50% (as measured in the practice EHR).
If you have the resources and opportunity, consider expanding the care team to help distribute new roles and responsibilities. The most common roles added to the care team include a community health worker and a behavioral health clinician. The community health worker can be trained to provide anticipatory guidance, parenting coaching, and child development support; conduct intake and screening processes; connect families with community resources; and/or provide care coordination and follow-up. The behavioral health clinician can provide evidence-based treatments that reduce the negative effects of trauma and increase resilience, including Child-Parent Psychotherapy,Child and Family Traumatic Stress Intervention, Trauma-Focused Cognitive Behavioral Therapy.48,49,50,51,52,53 Integrating the community health worker and the behavioral health clinician within the practice makes it possible to conduct warm hand-offs between these and other care team members.
You can learn more about the competencies and responsibilities of these roles when integrated into pediatric primary care with the following resources:
- Pediatric Integrated Primary Care an Implementation and Training Manual for Professionals (PDF – 1860 KB) - Children's Hospital Association
- HealthySteps Specialist Competencies and Related Resources - HealthySteps
- Early Childhood Support Specialist Evaluation Report - MaineHealth Health System
- Supporting Communication and Sharing Findings with Early Childhood Professionals - American Academy of Pediatrics
TIP: If you are unable to expand your care team to address gaps in knowledge, skills, and experience, up-train them instead.
Training care team members to perform new skills (up-training) can enable current care team members to provide anticipatory guidance, administer screening tools, connect families to community resources, or use data for quality improvement. For example, you can train staff on how to support families with transportation to medical appointments or respond to food insecurity by connecting parents to WIC, SNAP and local food pantries.
You can use the following tools to up-train care team members:
- Anticipatory Guidance Provider Guide (PDF – 1376 KB) - Texas Health and Human Services Commission
- Developmental Surveillance and Screening Educational Tools - American Academy of Pediatrics
Conduct training and education to increase staff and family understanding of trauma-informed care and how early childhood experiences, both positive and negative, can significantly impact a child's brain development and subsequent long-term health.
You can browse the resource collections below for existing materials for patient education and training or create your own:
- ACEs and Toxic Stress Patient Resource Library - ACEs Aware
- Well-Child Visits Parent and Patient Education Handouts - American Academy of Pediatrics
- HOPE Resource Library - Tufts Healthy Outcomes from Positive Experiences (HOPE)
You can browse the resource collections below for existing materials for provider education and training or create your own:
- Child Development Science Resource Library - Harvard University Center on the Developing Child
- Trauma Toolbox for Primary Care - American Academy of Pediatrics
- Mental Health Education and Training Tools - American Academy of Pediatrics
Select the screening tools and workflows your practice or system will use to identify children and families who have experienced trauma, developmental delays, and behavioral health symptomology and who have HRSN, such as transportation, housing, or food or diaper insecurity.
When implementing a new screening tool examine how the tool was validated. Most of the screening tools listed below were validated using a workflow where a parent or patient was provided the written questionnaire to self-complete. It is important to align your workflow as close as possible to the validated methodology for each tool that you choose to use. A common workflow error is to depend on clinical rooming staff to verbally ask screening questions as part of the vitals workflow. This type of misalignment can significantly affect the accuracy of screening tools.54,55,56,57
You can use this screening tool finder or the sample list below to identify validated screening tools for behavioral, social, and emotional health, child development, and HRSN for parents and caregivers with children ages 0-5 years. The list below is organized by screening tool type and child age.
- Early Childhood Developmental Screening Tools:
- The Survey of Well being of Young Children (SWYC) - Tufts Medicine. The SWYC includes sections on developmental milestones, behavioral/social-emotional development, and family risk-protective factors. (Ages 2 months through 5 years)
- ASQ-3 - Ages and Stages - The Ages & Stages Questionnaires®, Third Edition (ASQ®-3) is a developmental screening tool that measures developmental progress in young children. (Ages 1 month to 5½ years)
- Parents' Evaluation of Developmental Status (PEDS®) (PDF – 128 KB) - Minnesota Department of Education, Health, and Human Services. Screening tool that elicits and addresses parents' concerns about children's language, motor, self-help, early academic skills, behavior, and social-emotional/mental health. (Ages 0-8 years)
- Modified Checklist for Autism in Toddlers, Revised, with Follow-Up (M-CHAT-R/F) - Autism Speaks. The M-CHAT-R/F is a 2-stage parent-report screening tool to assess risk for Autism Spectrum Disorder. (Ages 16 to 30 months)
- Behavioral, Social, and Emotional Health Screening Tools
- Baby Pediatric Symptom Checklist (BPSC) - Tufts Medical Center. The BPSC is a brief social/emotional screening instrument. (Ages 0-18 months)
- Preschool Pediatric Symptom Checklist (PPSC) - Tufts Medical Center. The PPSC is a brief social/emotional screening instrument. (Ages 18 months through 5 years)
- Pediatric Symptom Checklist (PSC) - Massachusetts General Hospital. The Pediatric Symptom Checklist (PSC) is a brief screening questionnaire used by pediatricians and other health professionals to recognize psychosocial problems and improve treatment in children. (Ages 4-17 years)
- The Strengths and Difficulties Questionnaire (SDQ) - University of Washington. The Strengths and Difficulties Questionnaire (SDQ) is a brief behavioral screening questionnaire. There are several versions to meet the needs of researchers, clinicians, and educationalists. (Ages 2-17 years)
- Adversity-Trauma Screening
- Pediatric ACEs and Related Life Events Screener (PEARLS) (PDF – 187 KB) - ACES Aware. PEARLS identifies possible adverse childhood experiences and additional adversities that impact the growth and development of a child. (Ages 0-19 years)
- Parenting Stress Index-Short Form (PSI) - The National Child Traumatic Stress Network. The PSI is a screening and diagnostic assessment tool that can be used to measure stress in the parent-child system. (Ages 1 month to 12 years)
- SEEK – Safe Environment for Every Kid - The SEEK Project. SEEK screens parents for prevalent psychosocial problems that are risk factors for child maltreatment, and that generally jeopardize children's health, development, and safety. (Ages 1 to 65 months)
- Health-Related Social Needs Screening Tools
- MaineHealth Diaper Insecurity Mini Toolkit (PDF – 294 KB) - AHRQ Academy. (Ages 0-3 years)
- Accountable Health Communities Health-Related Social Needs Screening Tool (PDF – 328 KB) - Centers for Medicare & Medicaid Services. The Tool can help providers find out patients' needs in several core domains that community services can help with. (All ages)
- Screen and Intervene: A Toolkit for Pediatricians to Address Food Insecurity - Food Research and Action Center. (All pediatric ages)
- The Hunger Vital Sign: A New Standard of Care for Preventive Health - Children's Health Watch. The Hunger Vital Sign measures families' concerns about and access to food, much the way healthcare providers check other key vital signs, such as pulse and blood pressure. (All pediatric ages)
The resources below include sample workflows and scripts that you can use for screening:
- Provider Toolkit: Screening and Responding to the Impact of ACEs and Toxic Stress (PDF – 7.6 MB) - ACEs Aware
- Pediatric Behavioral-Developmental Health Screening Toolkit (PDF – 2.4 KB) - MaineHealth
- Screening for Adverse Childhood Experiences and Trauma: Technical Assistance Tool (PDF – 268 KB) -Center for Health Care Strategies
- Screening Sample Scripts for Pediatric Clinical Teams (PDF – 551 KB) - ACEs Aware
If you have not already, identify the government and community programs available to help you meet the needs of the families you serve. Your practice or system will not have the capacity to address every need identified during screening. Establishing direct relationships with these programs can further facilitate successful connections for families.
You can use this online social care database to find local community resources, including:
- Behavioral health
- Early intervention services
- Childcare agencies
- Preschool and early education
- Basic needs assistance
- Legal assistance
- Peer support
- Health and social services programs
For government resources and programs that help with food, housing, healthcare, and other basic living expenses, you can visit the following websites:
- Federal Government Benefits - U.S. General Services Administration
- State and Territory Financial Assistance for Families - Administration for Children and Families
- 211 (PDF – 104 KB) - Federal Communications Commission
Partner with your information technology staff to develop electronic health record (EHR) models capable of aligning workflow and data reports. Creating data-capturable fields early on can support the creation of essential EHR reports for tracking the rates of screening, positive risk identified, and interventions provided. Your practice or health system can use these reports to support implementing quality improvement methodologies for screening and response models—such as the Plan-Do-Study-Act (PDSA) cycle—and the data can also be used to create patient registries that provide increased supports and connections for families with higher barriers and adversity. You can determine if you are screening with fidelity and if you are responding as best as you can with the resources that you have. Additionally, your practice or health system can use these data tools to collect and process outcome data and monitor whether you are on track to reach the goals in your aim statements.
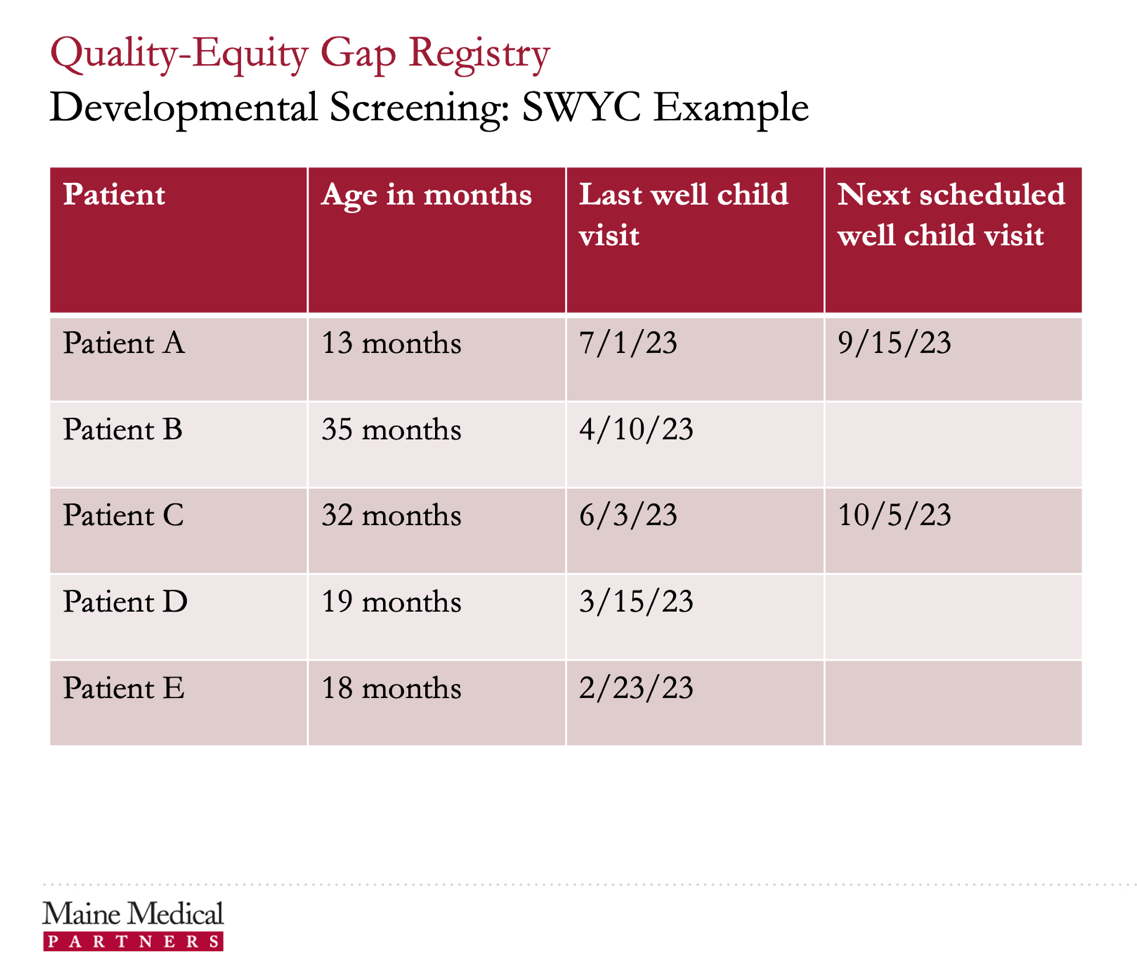
For instance, the example gap registry in Figure 1 (below) is based on Survey of Well-being of Young Children (SWYC) Developmental Screening Tool completion data in the EHR. The registry includes when the last well-child visit was and when the next one is scheduled. It answers the question: Who are the patients that did not get the recommended screening? If the patient has an upcoming appointment, front-line staff can be prepared to distribute the SWYC. If there is no appointment scheduled, then staff reach out to the family to schedule an appointment.
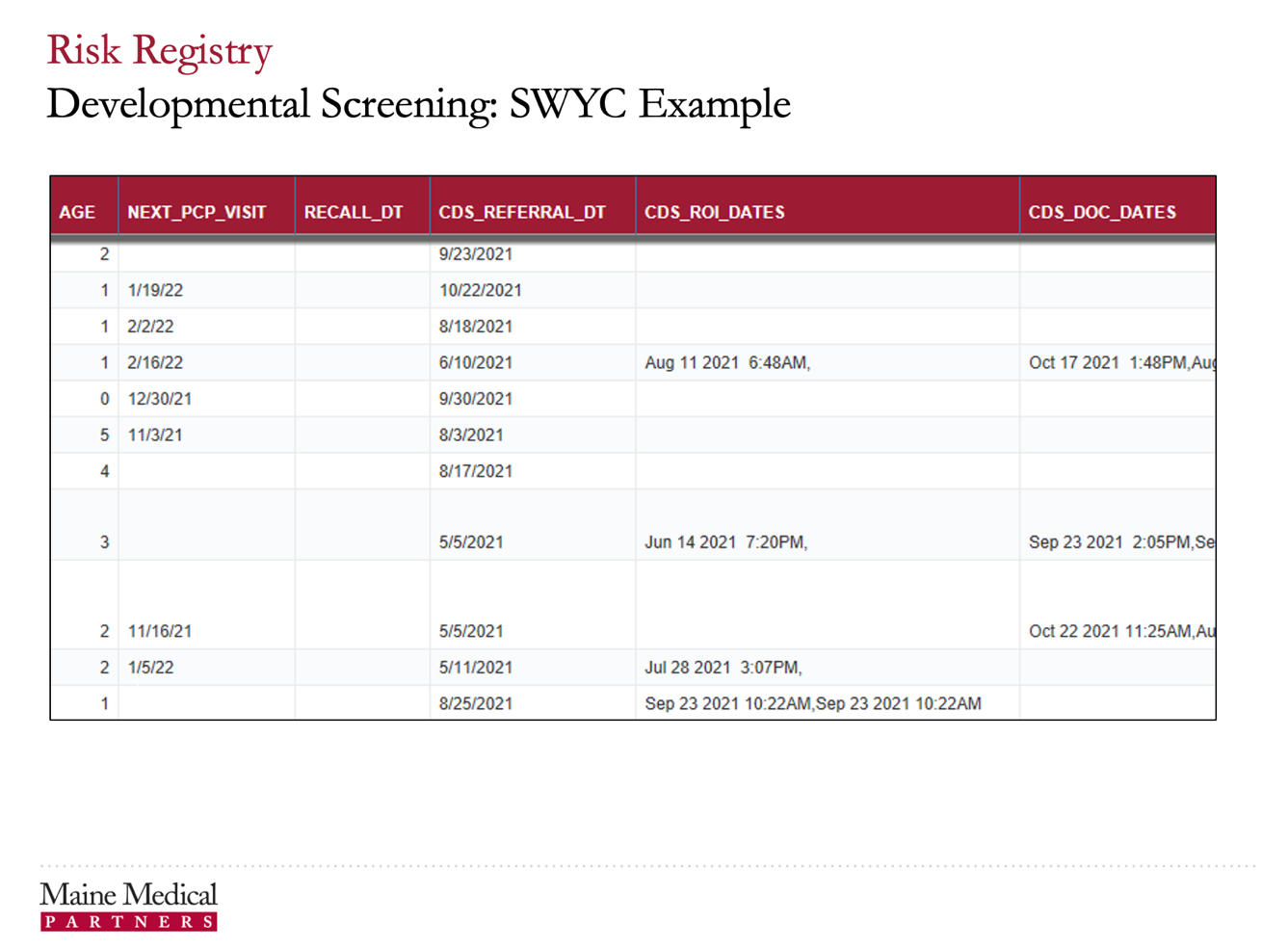
A screenshot of an exported electronic health record (EHR) report in the form of an Excel spreadsheet. This report is a risk registry for referrals to Child Developmental Services (CDS) based specifically on data captured via the Survey of Well-being of Young Children (SWYC) Developmental Screening Tool and stored in the EHR. The example shows a list of patients, eleven in total, represented by each row of the sheet. There is data on the patient’s age, next scheduled primary care provider visit, date the patient was referred to CDS, the date the release of information to CDS was obtained, and if documentation was received confirming the connection to CDS. The example shows that all patients have a date they were referred to CDS, but the practice has only received requests for release of information for five of those patients and only four have supporting documentation indicating they connected with CDS. The blanks on this spreadsheet indicate opportunities for team members to follow up to ensure the patient gets connected to CDS.
The example risk registry in Figure 2 (below) is based on completed SWYC screening tools. This registry identifies children who have developmental concerns and were referred to Child Developmental Services (CDS). The report identifies the date of the referral (CDS_REFERRAL_DT), if a release of information was obtained (CDS_ROI_DATES), and if documentation was received regarding the connection to CDS (CDS_DOC_DATES). When the connection is not completed, office staff or care management reach out to the parents or CDS to assist with connection.
A screenshot of an exported electronic health record (EHR) report in the form of an Excel spreadsheet. This report is a gaps-in-care registry based specifically on data captured via the Survey of Well-being of Young Children (SWYC) Developmental Screening Tool and stored in the EHR. The example shows a list of patients, their ages, when their last well child visit was scheduled and when the next one is scheduled. Three of the five included patients have a gap, indicated by no data, in the column for date of next scheduled well child visit. This indicates they do not have their next well child visit on the schedule, which is a care gap that a care team member would follow up on to address.
You can use the following resources to help with customizing EHRs:
- ACEs Aware Trauma-Informed Network of Care Roadmap: Characteristics of Effective Digital Health Resource Platforms (PDF – 4.8 MB) - ACEs Aware
- Adapting Electronic Health Records to Improve Trauma Screening and Referral Pathways (PDF – 268 KB) - Center for Health Care Strategies
- Improving the Rate of Mothers Reached During Referral Follow-Up Attempts (PDF – 1190 KB) - HealthySteps
- Behavioral-development health screening and response is an approach to pediatric primary care where care teams administer screenings to identify behavioral health symptomatology, developmental delays, adversity, and health-related social needs in children ages 0-5 and then provide brief interventions and referrals, if needed.
- While there is not yet an established and validated framework for this approach, several practices and health systems have developed their own models. Common components of these models include a trauma-informed approach, a two-generation approach, patient education, provider training, anticipatory guidance, team-based care, standardized screening and workflows, connections to community resources, and data utilization. Implementation of these components can be customized based on patient population, resources, staff expertise, and practice or system goals.
- Behavioral-developmental health screening and response models demonstrate promise in enhancing screening rates, identification of adversity, referrals to services, and patient satisfaction. While research is ongoing, initial findings from randomized control trials suggest that these models can reduce healthcare utilization, improve child development, and promote positive parenting practices. Further research is needed to fully establish the long-term impact on child and family outcomes.
- Pediatric and family medicine practices and health systems can implement behavioral-developmental health screening and response by setting goals, creating a training and education plan, adopting standardized tools and workflows, identifying community resources, redesigning and up-training the care team, and aligning EHRs to support workflows, data collection, and quality improvement.
Research on Behavioral-Developmental Health Screening and Response Model
- Center for the Study of Social Policy - Pediatrics Supporting Parents Program Analysis: Program and Site Selection Process and Results (PDF – 327 KB)
- Center for the Study of Social Policy - Fostering Social and Emotional Health through Pediatric Primary Care: Common Threads to Transform Everyday Practice and Systems (PDF – 1355 KB)
- Texas Children's Hospital - Expanding the Role of the Pediatric Practice: A Blueprint to Support Early Brain Development, Healthy Children, Stable Families, and Thriving Communities (PDF – 5.1 MB)
- Bipartisan Policy Center. The Science of Early Childhood Development. Washington, DC: Bipartisan Policy Center; October 2021. https://bipartisanpolicy.org/download/?file=/wp-content/uploads/2021/05/C.-1-The-Science-of-Early-Childhood.pdf (PDF - 144 KB). Accessed July 11, 2024.
- Harvard University Center on the Developing Child. InBrief: The Science of Early Childhood Development. https://developingchild.harvard.edu/resources/inbrief-science-of-ecd/. Accessed July 11, 2024.
- Maggi S, Irwin LJ, Siddiqi A, Hertzman C. The social determinants of early child development: an overview. Paediatr Child Health. 2010 Nov;46(11):627-35. https://doi.org/10.1111/j.1440-1754.2010.01817.x. Accessed July 11, 2024.
- National Scientific Council on the Developing Child. Excessive Stress Disrupts the Architecture of the Developing Brain. Working Paper No. 3. Cambridge, MA: Harvard University Center on the Developing Child; June 2009. https://edn.ne.gov/cms/sites/default/files/u1/pdf/se05SE2%20Stress%20Disrupts%20Architecture%20Dev%20Brain%203.pdf (PDF – 253 KB). Accessed July 11, 2024.
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, Marks JS. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998 May 1;14(4):245-58. https://www.ajpmonline.org/article/S0749-3797(98)00017-8/fulltext. Accessed July 11, 2024.
- Centers for Disease Control and Prevention. Adverse Childhood Experiences (ACEs): About Adverse Childhood Experiences. https://www.cdc.gov/aces/about/". Accessed July 11, 2024.
- Herzog JI, Schmahl C. Adverse childhood experiences and the consequences on neurobiological, psychosocial, and somatic conditions across the lifespan. Front Psychiatry. 2018 Sep 4;9:420. https://doi.org/10.3389/fpsyt.2018.00420. Accessed July 11, 2024.
- Substance Abuse and Mental Health Services Administration. Understanding Child Trauma. https://www.samhsa.gov/child-trauma/understanding-child-trauma. Accessed July 11, 2024.
- Anda RF, Felitti VJ, Bremner JD, Walker JD, Whitfield CH, Perry BD, Dube SR, Giles WH. The enduring effects of abuse and related adverse experiences in childhood: a convergence of evidence from neurobiology and epidemiology. Eur Arch Psychiatry Clin Neurosci. 2006 Apr;256:174-86. https://doi.org/10.1007%2Fs00406-005-0624-4. Accessed July 11, 2024.
- Slopen N, Koenen KC, Kubzansky LD. Cumulative adversity in childhood and emergent risk factors for long-term health. J Pediatr. 2014 Mar 1;164(3):631-8. https://doi.org/10.1016/j.jpeds.2013.11.003. Accessed July 11, 2024.
- Schwarzenberg SJ, Georgieff MK, Daniels S, Corkins M, Golden NH, Kim JH, Lindsey C, Magge SN. Advocacy for improving nutrition in the first 1000 days to support childhood development and adult health. Pediatrics. 2018 Feb 1;141(2). https://doi.org/10.1542/peds.2017-3716. Accessed August 11, 2024.
- Adalat S, Wall D, Goodyear H. Diaper dermatitis-frequency and contributory factors in hospital attending children. Pediatr Dermatol. 2007 Sep;24(5):483-8. https://doi.org/10.1111/j.1525-1470.2007.00499.x. Accessed August 11, 2024.
- Smith MV, Kruse A, Weir A, Goldblum J. Diaper need and its impact on child health. Pediatrics. 2013 Aug 1;132(2):253-9. https://doi.org/10.1542/peds.2013-0597. Accessed August 11, 2024.
- Huang CX, Halfon N, Sastry N, Chung PJ, Schickedanz A. Positive childhood experiences and adult health outcomes. Pediatrics. 2023 Jul 1;152(1):e2022060951. https://doi.org/10.1542/peds.2022-060951. Accessed August 11, 2024.
- Centers for Disease Control and Prevention. Adverse Childhood Experiences (ACEs): Risk and Protective Factors. https://www.cdc.gov/aces/risk-factors/index.html. Accessed July 11, 2024.
- Bethell C, Jones J, Gombojav N, Linkenbach J, Sege R. Positive childhood experiences and adult mental and relational health in a statewide sample: associations across adverse childhood experiences levels. JAMA Pediatr. 2019 Nov 1;173(11):e193007. https://doi.org/10.1001%2Fjamapediatrics.2019.3007. Accessed July 11, 2024.
- Kosterman R, Mason WA, Haggerty KP, Hawkins JD, Spoth R, Redmond C. Positive childhood experiences and positive adult functioning: prosocial continuity and the role of adolescent substance use. J Adolesc Health. 2011 Aug 1;49(2):180-6. https://doi.org/10.1016%2Fj.jadohealth.2010.11.244. Accessed July 11, 2024.
- Feldman R. What is resilience: an affiliative neuroscience approach. World Psychiatry. 2020 Jun;19(2):132-50. https://doi.org/10.1002/wps.20729. Accessed July 11, 2024.
- Bethell CD, Gombojav N, Whitaker RC. Family resilience and connection promote flourishing among US children, even amid adversity. Health Aff. 2019 May 1;38(5):729-37. https://doi.org/10.1377/hlthaff.2018.05425. Accessed July 11, 2024.
- Harvard University Center on the Developing Child. InBrief: Resilience Series. https://developingchild.harvard.edu/resources/inbrief-resilience-series/. Accessed July 11, 2024.
- Committee on Psychosocial Aspects of Child and Family Health, Committee on Early Childhood, Adoption, and Dependent Care, and Section on Developmental and Behavioral Pediatrics, Garner AS, Shonkoff JP, Siegel BS, Dobbins MI, Earls MF, Garner AS, McGuinn L, Pascoe J, Wood DL. Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics. 2012 Jan 1;129(1):e224-31. https://doi.org/10.1542/peds.2011-2662. Accessed July 11, 2024.
- Garner A, Yogman M, Committee on Psychosocial Aspects of Child and Family Health. Preventing childhood toxic stress: partnering with families and communities to promote relational health. Pediatrics. 2021 Aug 1;148(2). https://doi.org/10.1542/peds.2021-052582. Accessed July 11, 2024.
- Boudreau A, Hamling A, Pont E, Pendergrass TW, Richerson J. Pediatric primary health care: the central role of pediatricians in maintaining children's health in evolving health care models. Pediatrics. 2022 Feb 1;149(2):e2021055553. https://doi.org/10.1542/peds.2021-055553. Accessed July 11, 2024.
- ZERO TO THREE. Distillations: What does an early childhood professional do? https://www.zerotothree.org/resource/distillation/what-does-an-early-childhood-professional-do/. Accessed July 11, 2024.
- Bethell CD, Solloway MR, Guinosso S, Hassink S, Srivastav A, Ford D, Simpson LA. Prioritizing possibilities for child and family health: an agenda to address adverse childhood experiences and foster the social and emotional roots of well-being in pediatrics. Acad Pediatr. 2017 Sep 1;17(7):S36-50. https://doi.org/10.1016/j.acap.2017.06.002. Accessed July 11, 2024.
- Kerker BD, Storfer-Isser A, Szilagyi M, Stein RE, Garner AS, O'Connor KG, Hoagwood KE, Horwitz SM. Do pediatricians ask about adverse childhood experiences in pediatric primary care?. Acad Pediatr. 2016 Mar 1;16(2):154-60. https://doi.org/10.1016%2Fj.acap.2015.08.002. Accessed August 14, 2024.
- Committee on Psychosocial Aspects of Child and Family Health, Committee on Early Childhood, Adoption, and Dependent Care, and Section on Developmental and Behavioral Pediatrics, Garner AS, Shonkoff JP, Siegel BS, Dobbins MI, Earls MF, Garner AS, McGuinn L, Pascoe J, Wood DL. Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics. 2012 Jan 1;129(1):e224-31. https://doi.org/10.1542/peds.2011-2662. Accessed July 11, 2024.
- Garner A, Yogman M, Committee on Psychosocial Aspects of Child and Family Health. Preventing childhood toxic stress: partnering with families and communities to promote relational health. Pediatrics. 2021 Aug 1;148(2). https://doi.org/10.1542/peds.2021-052582. Accessed July 11, 2024.
- Liljenquist K, Coker TR. Transforming well-child care to meet the needs of families at the intersection of racism and poverty. Acad Pediatr. 2021 Nov 1;21(8):S102-7. https://doi.org/10.1016/j.acap.2021.08.004. Accessed July 11, 2024.
- Bethell CD, Solloway MR, Guinosso S, Hassink S, Srivastav A, Ford D, Simpson LA. Prioritizing possibilities for child and family health: an agenda to address adverse childhood experiences and foster the social and emotional roots of well-being in pediatrics. Acad Pediatr. 2017 Sep 1;17(7):S36-50. https://doi.org/10.1016/j.acap.2017.06.002. Accessed July 11, 2024.
- The Center for the Study of Social Policy. Pediatrics Supporting Parents: Program and Site Selection Process and Results. Washington, DC: Center for the Study of Social Policy; November 2019. https://cssp.org/wp-content/uploads/2025/03/PEDIATRIACS-SUPPORTING-PARENTS-MEMO.pdf (PDF – 327 KB). Accessed July 11, 2024.
- Doyle S, Chavez S, Cohen S, Morrison S. Fostering Social and Emotional Health through Pediatric Primary Care: Common Threads to Transform Everyday Practice and Systems—Executive Summary. Washington, DC: Center for the Study of Social Policy; September 2019. https://cssp.org/wp-content/uploads/2025/03/Fostering-Social-Emotional-Health-Full-Report.pdf (PDF- 987 KB). Accessed July 11, 2024.
- Correa N, Longmire-Jefferis V, Bhalakia AM, Cain C, Cummings A, Elango S, Greeley C, Killelea P, Lampe M, Lopez K, Mikhail O, Raphael JL, Ramphul R, Reiss J, Revere FL, Rodriguez LC, Sarpong K, Schwarzwald H, Tittle K, Usevitch M. Expanding the Role of the Pediatric Practice: A Blueprint to Support Early Brain Development, Healthy Children, Stable Families, and Thriving Communities. Houston, TX: Baylor College of Medicine and Texas Children's Hospital, November 2019. https://www.texaschildrens.org/sites/tc/files/2024-01/EHF-Expanded-Pediatric-Practice-Report-Final.pdf (PDF – 5.1 MB). Accessed July 11, 2024.
- Doyle S, Chavez S, Cohen S, Morrison S. Fostering Social and Emotional Health through Pediatric Primary Care: Common Threads to Transform Practice and Systems. Washington, DC: Center for the Study of Social Policy; September 2019. https://cssp.org/resource/fostering-social-emotional-health/". Accessed July 11, 2024.
- McBain RK, Levin JS, Matthews S, Qureshi N, Long D, Schickedanz AB, Gilgoff R, Kotz K, Slavich GM, Eberhart NK. The effect of adverse childhood experience training, screening, and response in primary care: a systematic review. EClinicalMedicine. 2023 Nov 1;65. https://doi.org/10.1016%2Fj.eclinm.2023.102282. Accessed July 11, 2024.
- Loveday S, Hall T, Constable L, Paton K, Sanci L, Goldfeld S, Hiscock H. Screening for adverse childhood experiences in children: a systematic review. Pediatrics. 2022 Feb 1;149(2):e2021051884. https://doi.org/10.1542/peds.2021-051884. Accessed July 11, 2024.
- Thornton RL, Yang TJ. Addressing population health inequities: investing in the social determinants of health for children and families to advance child health equity. Curr Opin Pediatr. 2023 Feb 1;35(1):8-13. https://doi.org/10.1097%2FMOP.0000000000001189. Accessed July 11, 2024.
- Sege R, Preer G, Morton SJ, Cabral H, Morakinyo O, Lee V, Abreu C, De Vos E, Kaplan-Sanoff M. Medical-legal strategies to improve infant health care: a randomized trial. Pediatrics. 2015 Jul 1;136(1):97-106. https://doi.org/10.1542/peds.2014-2955. Accessed July 11, 2024.
- Dodge KA, Goodman WB, Murphy RA, O'Donnell K, Sato J. Randomized controlled trial of universal postnatal nurse home visiting: impact on emergency care. Pediatrics. 2013 Nov 1;132(Supplement_2):S140-6. https://doi.org/10.1542/peds.2013-1021M. Accessed August 11, 2024.
- Goodman WB, Dodge KA, Bai Y, O'Donnell KJ, Murphy RA. Randomized controlled trial of Family Connects: effects on child emergency medical care from birth to 24 months. Dev Psychopathol. 2019 Dec;31(5):1863-72. https://doi.org/10.1017/S0954579419000889. Accessed August 11, 2024.
- Dodge KA, Goodman WB, Bai Y, O'Donnell K, Murphy RA. Effect of a community agency–administered nurse home visitation program on program use and maternal and infant health outcomes: a randomized clinical trial. JAMA Netw Open. 2019 Nov 1;2(11):e1914522-. https://doi.org/10.1001/jamanetworkopen.2019.14522. Accessed July 11, 2024.
- Minkovitz C, Strobino D, Hughart N, Scharfstein D, Guyer B, Healthy Steps Evaluation Team. Early effects of the healthy steps for young children program. Arch Pediatr Adolesc Med. 2001 Apr 1;155(4):470-9. https://doi.org/10.1001/archpedi.155.4.470. Accessed August 11, 2024.
- Valado T, Tracey J, Goldfinger J, Briggs R. HealthySteps. HealthySteps: transforming the promise of pediatric care. The Future of Children. 2019 Apr 1;29(1):99-122. https://files.eric.ed.gov/fulltext/EJ1220075.pdf (PDF – 275 KB). Accessed August 11, 2024.
- Coker TR, Chacon S, Elliott MN, Bruno Y, Chavis T, Biely C, Bethell CD, Contreras S, Mimila NA, Mercado J, Chung PJ. A parent coach model for well-child care among low-income children: a randomized controlled trial. Pediatrics. 2016 Mar 1;137(3). https://doi.org/10.1542%2Fpeds.2015-3013. Accessed July 11, 2024.
- Coker TR, Liljenquist K, Lowry SJ, Fiscella K, Weaver MR, Ortiz J, LaFontaine R, Silva J, Salaguinto T, Johnson G, Friesema L. Community health workers in early childhood well-child care for medicaid-insured children: a randomized clinical trial. JAMA. 2023 May 23;329(20):1757-67. https://doi.org/10.1001%2Fjama.2023.7197. Accessed July 11, 2024.
- Dubowitz H, Feigelman S, Lane W, Kim J. Pediatric primary care to help prevent child maltreatment: the Safe Environment for Every Kid (SEEK) Model. Pediatrics. 2009 Mar 1;123(3):858-64. https://doi.org/10.1542/peds.2008-1376. Accessed July 11, 2024.
- Dubowitz H, Lane WG, Semiatin JN, Magder LS. The SEEK model of pediatric primary care: can child maltreatment be prevented in a low-risk population?. Acad Pediatr. 2012 Jul 1;12(4):259-68. https://doi.org/10.1016/j.acap.2012.03.005. Accessed July 11, 2024.
- Trauma-Focused Cognitive Behavioral Therapy National Therapist Certification Program. Randomized Clinical Trials. https://tfcbt.org/randomized-clinical-trials/. Accessed July 11, 2024.
- Lieberman AF, Ippen CG, Van Horn P. Child-parent psychotherapy: 6-month follow-up of a randomized controlled trial. J Am Acad Child Adolesc Psychiatry. 2006 Aug 1;45(8):913-8. https://doi.org/10.1097/01.chi.0000222784.03735.92. Accessed July 11, 2024.
- Luby JL, Barch DM, Whalen D, Tillman R, Freedland KE. A randomized controlled trial of parent-child psychotherapy targeting emotion development for early childhood depression. Am J Psychiatry. 2018 Nov 1;175(11):1102-10. https://doi.org/10.1176/appi.ajp.2018.18030321. Accessed July 11, 2024.
- Hagan MJ, Browne DT, Sulik M, Ippen CG, Bush N, Lieberman AF. Parent and child trauma symptoms during child–parent psychotherapy: a prospective cohort study of dyadic change. J Trauma Stress. 2017 Dec;30(6):690-7. https://doi.org/10.1002/jts.22240. Accessed July 11, 2024.
- Yale School of Medicine Child Study Center. Child and Family Traumatic Stress Intervention. https://medicine.yale.edu/childstudy/services/community-and-schools-programs/yctsr/stress-intervention/. Accessed July 11, 2024.
- Berkowitz SJ, Stover CS, Marans SR. The child and family traumatic stress intervention: secondary prevention for youth at risk of developing PTSD. J Child Psychol Psychiatry. 2011 Jun;52(6):676-85. https://doi.org/10.1111/j.1469-7610.2010.02321.x. Accessed July 11, 2024.
- DiGiovanni SS, Frances RJ, Brown RS, Wilkinson BT, Coates GE, Faherty LJ, Craig AK, Andrews ER, Gabrielson SM. Pediatric trauma and posttraumatic symptom screening at well-child visits. Pediatr Qual Saf. 2023 May 1;8(3):e640. https://doi.org/10.1097%2Fpq9.0000000000000640. Accessed July 11, 2024.
- Ford J, Thomas F, Byng R, McCabe R. Use of the Patient Health Questionnaire (PHQ-9) in practice: interactions between patients and physicians. Qual Health Res. 2020 Nov;30(13):2146-59. https://doi.org/10.1177/1049732320924625. Accessed August 14, 2024.
- New York State Department of Health. Administering the Patient Health Questionnaires 2 and 9 (PHQ 2 and 9) in Integrated Care Settings. https://www.health.ny.gov/health_care/medicaid/redesign/dsrip/2016-07-01_phq_2_and_9_clean.htm. Accessed August 14, 2024.
- Policy Lab at the Children's Hospital of Philadelphia. Food for Thought: How We Screen for Food Insecurity Matters. https://policylab.chop.edu/blog/food-thought-how-we-screen-food-insecurity-matters. Accessed August 14, 2024.
Authors
- Monique Thornton, MPH - CEO, Let's Talk Public Health
- Steven DiGiovanni, MD - Medical Director for the Maine Medical Center Outpatient Clinics and Medical Lead for the MaineHealth Adverse Childhood Experiences (ACEs) and Resiliency Program
Other Contributors
- Garrett E. Moran, PhD - Principal, Moran Consulting
- Alec Hester, BS - Research Associate, Westat
- Danielle Durant, PhD, MS, MS, MBA - Principal Research Associate, Westat
Acknowledgements
We thank reviewers and other contributors from the Agency of Healthcare Quality and Research (AHRQ), National Integration Academy Council (NIAC), and Westat for sharing their time and expertise to develop, improve, and publish this work
Suggested Citation
Thornton M, DiGiovanni S. The Role of Behavioral-Developmental Health Screening and Response for Children Ages 0-5 in Pediatric Primary Care. Rockville, MD: Agency for Healthcare Research and Quality; September 2024. https://integrationacademy.ahrq.gov/products/topic-briefs/age-0-5-behavioral-development.